


Most pharma and biotech IT estates have already migrated. The major cloud platforms now offer regulated-environment configurations, BAA coverage, and validated reference architectures for clinical, regulatory, and commercial workloads. Raw cloud capacity, however, does not solve the operational problems life sciences teams actually feel: clinical teams still spend a disproportionate share of their time searching for protocol documents, screening patients for trials, and reconciling case report forms. Pharmacovigilance teams process growing volumes of adverse event reports under tight regulatory windows; the U.S. FDA’s FAERS database now contains over 31 million adverse event reports, with intake volumes climbing year over year . Regulatory affairs teams still hand-curate submission narratives across thousands of pages.
What "augmentative" actually means in life sciences
The seven categories of augmentative tools worth evaluating
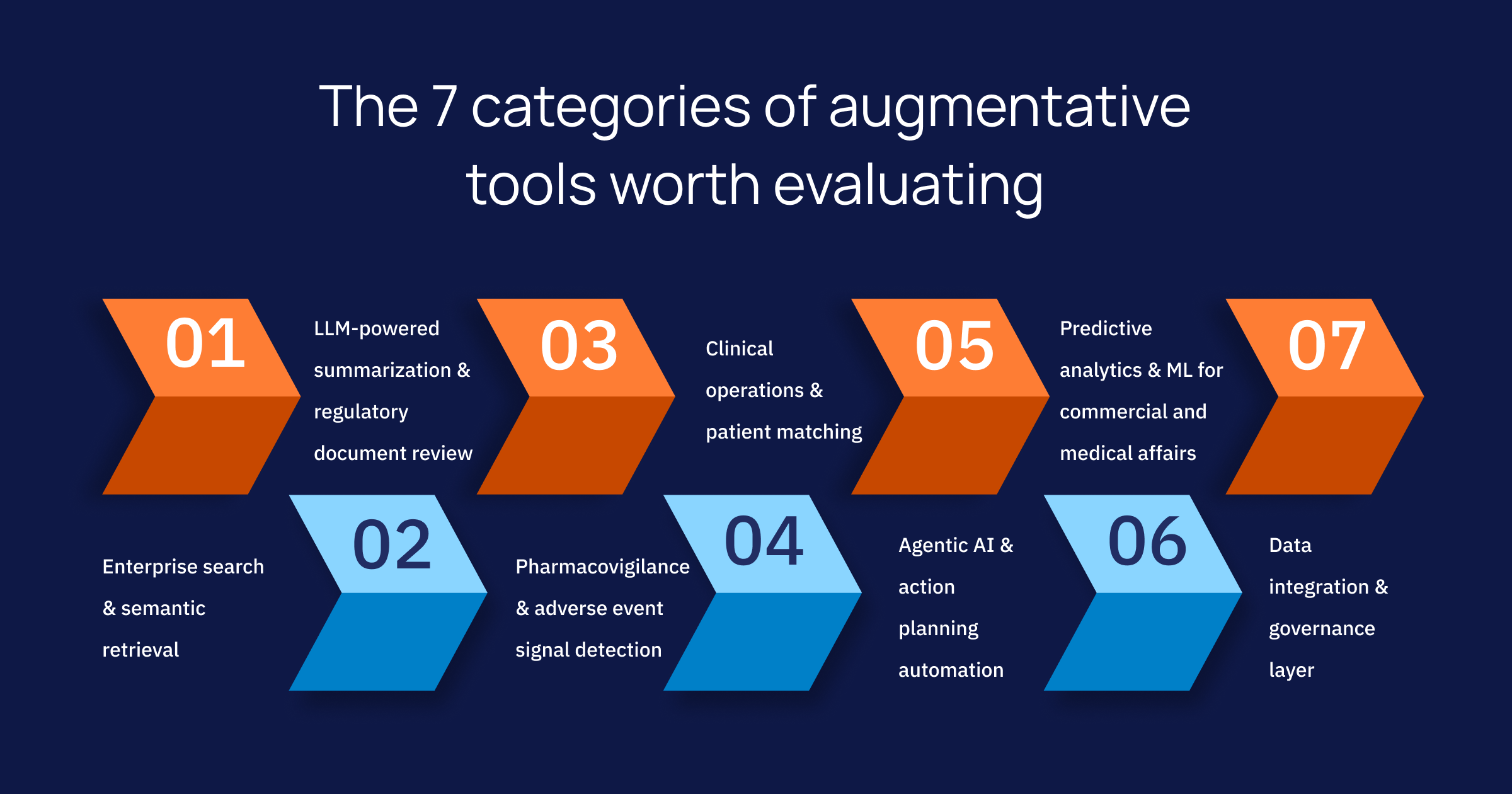
1. Enterprise search and semantic retrieval
2. LLM-powered summarization and regulatory document review
3. Pharmacovigilance and adverse event signal detection
While the AE intake volume continues to compound annually, the PV team headcount usually cannot match that pace. Augmentative tools here perform case intake from unstructured text, MedDRA coding suggestions, duplicate detection, and signal triage across product portfolios. The combination of NLP, classification models, and rules-driven validation is where most production deployments have settled.
4. Clinical operations and patient matching
5. Agentic AI and action planning automation
6. Predictive analytics and ML for commercial and medical affairs
7. Data integration and governance layer
How to choose AI tools that integrate with a life science cloud platform
| Evaluation lens | What to verify |
|---|---|
| Regulatory fit | Validated against 21 CFR Part 11, EU GMP Annex 11, GxP, and HIPAA. Audit trails on prompts, outputs, and model versions. |
| Data residency & isolation | BAA coverage, private model deployment, no training on customer data, regional data residency for EU/UK/APAC studies. |
| Integration depth | Native connectors to Veeva Vault, Salesforce Health Cloud, AWS HealthLake, Azure Health Data Services, Snowflake, Databricks, EHR FHIR endpoints. |
| Explainability | Citations on every generated answer, traceable retrieval paths, model cards, and documented evaluation on life sciences corpora. |
| Human-in-the-loop design | Review gates, role-based approval, controlled rollback, and the ability to disable autonomous actions in regulated workflows. |
| Total cost of ownership | Inference costs at production volumes, model-update cadence, and the operational overhead of maintaining prompt and retrieval pipelines. |
Where augmentation tends to break
How Intuceo augments your cloud-based life science environment
- Neural enterprise search (Intuceo-Ix™) : retrieval across LIMS, PLM, SharePoint, clinical archives, and FDA filings, adapted to your repositories rather than rebuilt from zero.
- Agentic BI (Intuceo-Ax™) : natural-language interrogation of clinical, regulatory, and commercial KPIs.
- Clinical and patient-facing agents (AgentCare AI) : trial matching, AE intake, and care orchestration patterns proven in earlier engagements.
- Adverse event detection (AE Detection) : classification, MedDRA coding suggestions, and signal triage tuned for pharmacovigilance teams.
- Clinical Trial Patient Matching : LangGraph-orchestrated matching with SNOMED CT entity resolution against EHR cohorts.
- iPDLC™ delivery framework : our delivery lifecycle for HIPAA, FISMA, 21 CFR Part 11, and GxP audit-readiness, so validation is built into the engagement rather than bolted on at the end.
Build Your Augmentation Roadmap
Frequently Asked Questions
1.Which AI tools are best for a cloud-based life science platform?
2.Which tools help with compliant AI in pharma and biotech?
3.What tools help with summarization, search, and action planning in life sciences?
Summarization is best handled by LLMs fine-tuned or grounded against life sciences corpora with retrieval-augmented generation. Search requires semantic and vector retrieval across structured and unstructured repositories. Action planning automation sits on top of both, using agentic frameworks to execute multi-step workflows and surface exceptions to human reviewers.