


A researcher at a pharmaceutical company needs specific safety data from a clinical trial conducted eight years ago. The information exists, but it is fragmented across regulatory filings, Clinical Study Reports (CSRs), and investigator brochures, scattered across SharePoint, a LIMS, and two legacy Document Management Systems (DMS). What should be a precise query becomes a time-consuming manual audit.
This is not an edge case; it is a systemic operational bottleneck. As clinical document repositories scale, they have evolved into “data graveyards” rather than active knowledge bases. With healthcare data volumes growing at 36% annually, outpacing both manufacturing and finance, the infrastructure used to store this data is crumbling under the weight of its own complexity.
The root of this bottleneck extends beyond simple indexing issues. It is the result of deep-seated technical hurdles: fragmented data silos, a lack of standardized metadata, and the inherent difficulty of querying unstructured text within massive, non-machine-readable PDFs. When retrieval lags, the consequences extend beyond mere frustration – they manifest as delayed regulatory responses, compromised patient safety insights, and decision cycles that cannot keep pace with the speed of modern drug development.
$2.59B
AutoML global market value in 2025
41.96%
CAGR projected through 2031
Why Clinical Document Search Systems Fail at Scale
Retrieval latency in large clinical document repositories is rarely caused by a single factor. It compounds across several dimensions.
Unstructured Data Without Standardization
Life science organizations generate massive volumes of unstructured clinical data: handwritten physician notes, scanned regulatory submissions, multi-format trial reports, pathology narratives, and adverse event case files. This data lacks the structured schemas that conventional databases rely on. Without standardized tagging or formatting, search systems cannot index content meaningfully. A 2019 PMC study confirmed that approximately 80% of medical data remains unstructured and untapped after creation, with most hospital information systems unable to process it effectively.
Poor Document Chunking Strategies
When organizations feed clinical PDFs and regulatory filings into modern search or retrieval augmented generation (RAG) systems, document chunking becomes a critical failure point. Fixed-size chunking, the most common default, splits documents at arbitrary character counts without regard for section boundaries, tables, or clinical context. A chunk that starts mid-paragraph in a pharmacokinetics section and ends in an adverse event summary returns contextually meaningless results.
Effective chunking for clinical documents requires structural awareness, recognizing that a protocol synopsis is a single logical unit while a multi-page adverse event narrative must be segmented by case, not by page count.
Keyword Search Cannot Handle Clinical Complexity
Traditional keyword-based search breaks down in clinical repositories because medical language is inherently ambiguous. A clinician searching for “heart failure management” may need results that reference “CHF protocols,” “left ventricular dysfunction interventions,” or “HFrEF treatment guidelines,” none of which share the original keywords.
A 2025 systematic literature review of RAG in healthcare identified retrieval noise (irrelevant or low-quality retrieved information), inference latency, domain shift, and limited interpretability as persistent challenges in clinical retrieval systems. Semantic search addresses this by matching intent rather than exact terms, but many life science organizations still rely on legacy keyword engines.
Siloed Systems and Fragmented Repositories
Clinical knowledge rarely lives in one place. Trial data sits in an EDC system. Regulatory correspondence lives in a separate document management platform. Lab results are locked inside LIMS. Each system has its own access controls, metadata schemas, and search interfaces. This fragmentation forces knowledge workers to run parallel searches across disconnected platforms.
According to McKinsey, employees spend an average of 1.8 hours per day searching for and gathering information. In regulated life science environments, where document retrieval involves cross-referencing multiple systems for audit or submission purposes, that number runs highe
Missing Metadata and Taxonomy Gaps
Metadata is the backbone of fast, accurate retrieval. Without proper metadata enrichment, including document type, therapeutic area, study phase, and regulatory jurisdiction, search engines cannot surface the right results. Many clinical repositories were built over decades, and legacy documents were ingested without consistent tagging. When a repository holds millions of pages across disparate archives, missing metadata creates blind spots that no amount of search tuning can fix.
OCR Limitations on Scanned Clinical Documents
A significant portion of clinical repositories includes scanned documents: legacy trial reports, handwritten clinical notes, signed regulatory forms, and faxed correspondence. Standard OCR introduces errors that propagate through every downstream search query. Misread characters in drug names, dosage figures, or patient identifiers make these documents effectively invisible to retrieval systems. Poor PDF OCR search quality is a silent contributor to retrieval failures that organizations often underestimate.
The scale of the problem: Healthcare organizations are storing upwards of 50+ petabytes of data, retained for decades to meet compliance requirements. This data is difficult to manage, search, and analyze using standard tools.
Proven Solutions for Faster, More Accurate Clinical Document Retrieval
Addressing retrieval latency in clinical repositories requires a layered approach that tackles data quality, search architecture, and knowledge organization simultaneously.
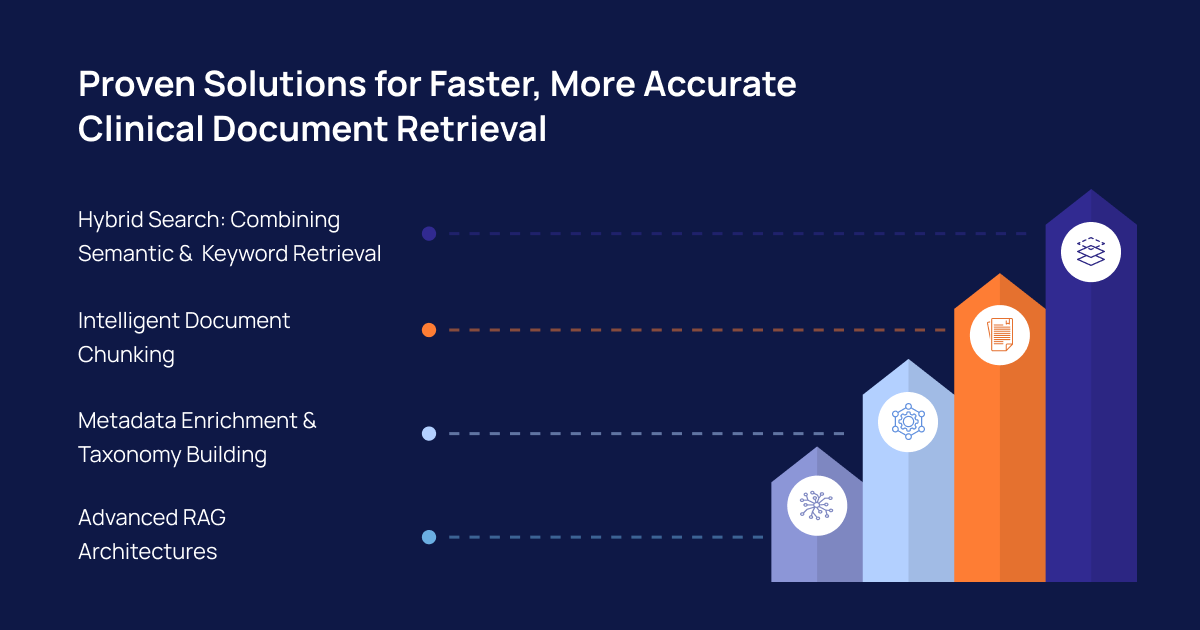
Hybrid Search: Combining Semantic and Keyword Retrieval
Neither pure keyword search nor pure semantic search is sufficient for clinical repositories. Hybrid search combines sparse retrieval (BM25-based keyword matching) with dense retrieval (neural embedding-based semantic matching) to capture both exact clinical terms and conceptual equivalents.
A 2025 study evaluating RAG variants for clinical decision support found that while a Haystack pipeline (DPR + BM25 + cross encoder) and hybrid fusion (RRF) delivered the best retrieval accuracy, self-reflective RAG reduced hallucinations to 5.8%.
The optimal architecture layers both, using keyword matching for precise regulatory terms and semantic search for broader clinical concepts.
Metadata Enrichment and Taxonomy Building
Retroactive metadata enrichment using NLP-based entity extraction and classification models transforms previously unsearchable archives into queryable knowledge bases. Building a controlled taxonomy specific to the organization’s therapeutic areas and regulatory frameworks ensures search systems map user queries to correct document categories, which is critical for life science information retrieval across multi-decade archives.
Advanced RAG Architectures
Retrieval augmented generation is emerging as a critical capability for clinical knowledge retrieval systems. RAG pipelines retrieve relevant document chunks and feed them to a language model that synthesizes a grounded, contextual answer. For healthcare, this improves factual consistency and reduces hallucinations compared to standalone LLMs. However, RAG for clinical documents requires careful attention to retrieval quality; if the underlying search returns noisy chunks, the generated output inherits those errors.
How Intuceo Solves Clinical Document Retrieval at Scale
Intuceo has engineered purpose-built solutions for exactly this challenge. Intuceo-Ix™ (Neural Search Intelligence) goes beyond keyword matching to provide neural semantic discovery across fragmented institutional silos, reducing information retrieval time by 70%. Its InsightExplorer™ interface enables researchers and knowledge workers to query millions of records with sub-second response times.
For organizations dealing with legacy scanned documents and handwritten clinical notes, Intuceo-Dx™ (Document & Vision Intelligence) uses Vision AI to extract high-fidelity metadata that traditional OCR misses, converting complex analog documentation into structured, searchable records. Its RAG-enabled extraction capability lets teams query their document library as if it were a live expert.
In one engagement, Intuceo deployed a Universal Search Engine that indexed 5M+ documents across SharePoint, LIMS, PLM, clinical trials, FDA filings, and patents, transforming R&D workflows and reducing information discovery time from 90% of a knowledge worker’s day to just 10%.
All Intuceo solutions are deployed within air-gapped, HIPAA-compliant environments. No client data is used to train public models. The intelligence generated remains 100% proprietary.
All Intuceo solutions are deployed within air-gapped, HIPAA-compliant environments. No client data is used to train public models. The intelligence generated remains 100% proprietary.
Frequently Asked Questions
1.Why is retrieval so slow in large clinical document repositories?
Retrieval slows down due to massive volumes of unstructured clinical data, fragmented storage across multiple systems (EDC, LIMS, QMS, SharePoint), inconsistent or missing metadata, poor document chunking, and reliance on keyword-only search engines that cannot interpret clinical terminology variations.
2.What causes poor retrieval accuracy in healthcare RAG systems?
The most common causes are retrieval noise from poorly chunked documents, domain shift when embedding models are not tuned for clinical vocabulary, and incomplete metadata that prevents the retriever from narrowing results effectively. A RAG system is only as good as the documents it retrieves.
3.What is the best chunking strategy for medical or clinical documents?
Structure-aware chunking outperforms fixed-size approaches. This involves parsing documents into logical clinical sections (safety narratives, protocol amendments, pharmacokinetic summaries) and enriching each chunk with extracted entities such as drug names, conditions, and study identifiers.
4.How do metadata and taxonomy improve retrieval in life science repositories?
Metadata provides the filtering and categorization layer that search engines need. A well-built taxonomy maps organizational vocabulary to standardized clinical terms, ensuring queries for “adverse event reports” also surface documents tagged under “safety signals” or “AER classifications.”
5.How can LLMs handle long clinical documents more effectively?
The most effective approach combines intelligent chunking, entity-enriched indexing, and RAG architectures that retrieve only the most relevant segments before passing them to the model for synthesis. This keeps responses grounded in specific evidence rather than diluted across thousands of pages.