


A landmark study of roughly 100 million patient encounters found that physicians spend an average of 16 minutes and 14 seconds inside the electronic health record (EHR) per visit, with chart review alone accounting for 33% of that time, the single largest category.[1] A significant share of those minutes is not reading; it is searching. Clinicians scroll, click between tabs, and reopen the same folders, trying to surface one prior note. Slow clinical document retrieval EHR workflows quietly tax every encounter. Most pharmaceutical organizations now generate real-world evidence. However, only a few have wired it into the daily decisions of clinical, medical, and commercial teams.
This article breaks down why retrieval drags, why conventional search hits a ceiling, and the approaches that move EHR document retrieval time from minutes back toward seconds, without pretending the fix is a single switch.
Key Takeaways
- Chart review is the largest single consumer of clinician EHR time, so even small gains in patient document retrieval EHR speed compound across thousands of encounters.
- Since a huge chunk of clinical data sits in unstructured free text, which exact-match and keyword queries cannot search well, the root cause behind most slow EHR document retrieval.
- Conventional structured queries match characters, not meaning; semantic, artificial intelligence (AI)-assisted retrieval matches intent, which is why it changes clinical database search performance.
- Lasting clinical document search optimization combines proper indexing, text extraction from scanned files, and governed access, not a faster server alone.
- In regulated healthcare settings, any retrieval improvement has to preserve Health Insurance Portability and Accountability Act (HIPAA) safeguards, audit trails, and access controls by design.
What Actually Causes Slow Clinical Document Retrieval
Sluggish retrieval rarely traces back to a single mistake. It usually stems from several compounding ones.
Volume and sprawl
A single longitudinal record can hold thousands of documents accumulated across years, encounters, and care settings. As repositories grow, naive queries that scan ever-larger tables degrade, and the EHR system document loading speed falls with them. Fragmentation makes it worse: records often span multiple connected systems, so a single retrieval touches several stores before anything renders.
The unstructured text problem
Most of the clinical story lives in narrative. Across the research literature, roughly 80% of EHR data is unstructured free text such as progress notes, discharge summaries, and radiology reports.[2] Structured fields like diagnosis codes index cleanly. Free text does not, so when a clinician needs the note where a specific symptom was first described, an exact-match search has little to grip.
Scanned and imaged documents
Outside referrals, faxed forms, and historical charts frequently enter the repository as images. Without text extraction, they are invisible to any query, which means part of the record cannot be retrieved at all, only browsed for manually.
Indexing gaps
Where indexes are missing, stale, or poorly chosen for how clinicians actually search, the database falls back to slow scans. Weak clinical document indexing speed is one of the most common and most fixable bottlenecks in the chain.
Why Conventional Search Hits a Ceiling
This is where the difference between traditional and AI-assisted retrieval becomes concrete. A structured query, the kind written in SQL (Structured Query Language) against indexed fields, is fast and precise when you know the exact code, date, or field to ask for. It matches characters. Ask it for “shortness of breath,” and it will miss the note that says “dyspnea,” “SOB,” or “patient winded on exertion,” because none of those strings match. For coded, tabular data, structured search is the right tool. For the free-text majority of the record, it leaves most of the content unreachable.
Layering more keyword filters does not solve this. It pushes the clinician toward guessing the precise wording a colleague happened to type months earlier. The ceiling is not server speed; it is that exact-match logic cannot understand clinical meaning. Real healthcare document retrieval optimization has to close the gap between what a clinician means and what a query can match.
How Semantic, AI-Assisted Retrieval Changes the Picture
Semantic search takes a different route. Instead of matching strings, it converts documents and queries into numerical representations of meaning, so a search for “shortness of breath” surfaces “dyspnea” and “SOB” because the concepts sit close together, regardless of wording. Large language models (LLMs) and clinical natural language processing extend this further: they read narrative text, recognize medical concepts and their synonyms, and rank results by relevance to the clinical question rather than by literal overlap.
Three capabilities do most of the work in practice.
- First, text extraction turns scanned and imaged documents into searchable content, pulling the invisible part of the record into reach.
- Second, concept-aware indexing builds an index around meaning, so retrieval no longer depends on the clinician guessing exact phrasing.
- Third, relevance ranking returns the few documents that answer the question first, instead of a long, undifferentiated list.
Together, these address the unstructured-text problem at its source and lift EHR repository performance in the way clinicians feel most: the right note appears near the top, fast.
The aim is not to replace structured queries. Coded fields still belong in fast structured search. The point is to add a meaning-aware path for the narrative majority of the record, so both kinds of questions get answered well.
Practical Steps That Speed Up Retrieval
Moving from diagnosis to measurable improvement follows a consistent sequence.
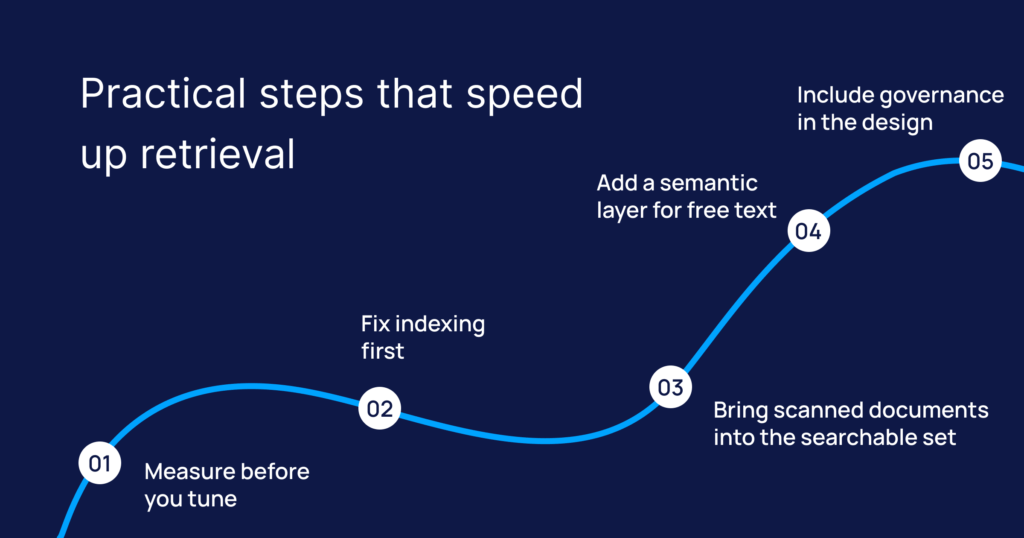
Measure before you tune.
Capture real retrieval times for the queries clinicians run most, then rank them by frequency and pain. Without those baseline numbers, you have no way to tell whether a change actually made electronic health record document retrieval faster, and the worst offenders are rarely the ones teams assume.
Fix indexing first
Review and rebuild indexes around genuine search patterns. This is frequently the highest-return, lowest-disruption step, and it often recovers a large share of lost speed before any advanced tooling enters the picture.
Bring scanned documents into the searchable set
Run text extraction across imaged and faxed files so the full record becomes retrievable rather than merely piling up on the data pool.
Add a semantic layer for free text
Introduce concept-aware search over narrative notes so meaning-based queries work alongside structured ones. This is the step that most directly drives clinical document search optimization for the unstructured majority.
Include governance in the design
Every improvement must respect role-based access, full audit logging, and patient privacy obligations from the first build, because retrofitting controls into a live retrieval pipeline is slow, costly, and risky.
Where Intuceo Fits: Services That Make the Record Findable
Intuceo is a PhD-led AI, machine learning, and data analytics services firm with deep experience inside regulated healthcare environments, including engagements with organizations such as UF Health (University of Florida Health), Florida Blue, and Guidewell Health.
Our teams diagnose where retrieval actually breaks down in a given repository, then build and configure the fix.
Intuceo-Ix™, our semantic and neural search accelerator, brings concept-aware retrieval across millions of indexed clinical documents so a query for one idea surfaces every way clinicians phrased it.
Intuceo-Dx™, our document and vision intelligence accelerator, extracts text from scanned referrals, faxes, and historical charts, so the imaged portion of the record is no longer a blind spot.
These are accelerators that a services team carries in from prior healthcare work and tunes to your systems, not off-the-shelf installs, and every engagement is delivered with HIPAA, HITRUST (Health Information Trust Alliance), and SOC 2 Type II (System and Organization Controls) safeguards built into the work.
The result clinicians notice is simple: the right document, surfaced in seconds, with the access trail intact.
How Long Does Retrieval Take in Your Repository?
Talk to Intuceo’s PhD-led team about a focused assessment of your EHR retrieval workflows: where is the team’s time going, which documents are hidden, and the shortest compliant path to surfacing them in seconds.
Frequently Asked Questions
1.What causes slow clinical document retrieval in EHR repositories?
Usually, a combination: large and fragmented record volumes, missing or stale indexes, and the fact that most clinical content is unstructured free text that exact-match search handles poorly. Scanned documents with no extracted text add a further layer, since they cannot be queried at all.
2.What is the difference between SQL and LLM-based EHR document search?
A SQL-style structured query matches exact values in indexed fields and is excellent for coded data such as diagnosis codes and dates. An approach using large language models and semantic search matches meaning, so it retrieves clinically equivalent terms and reads narrative notes. The two are complementary: structured search for coded fields, meaning-aware search for free text.
3.Can large language models improve EHR repository performance?
For the unstructured majority of the record, yes. Language models and clinical natural language processing recognize concepts, synonyms, and context, so relevant notes surface even when wording differs. They do not replace structured queries for coded data; they add a meaning-aware path for narrative content that keyword search misses.
4.How do I reduce clinical document retrieval time from minutes to seconds?
Measure your slowest high-frequency queries, fix indexing around real search patterns, extract text from scanned files, and add a semantic search capability over free text. Most programs see the largest early gains from indexing work, with semantic retrieval addressing the queries that structured search could never answer.
5.What are the main bottlenecks in clinical document retrieval workflows?
The recurring ones are unindexed or poorly indexed content, unstructured text that resists keyword search, imaged documents with no extracted text, and records fragmented across connected systems. Governance gaps can also slow things down when access checks are inefficient or applied inconsistently.