
Enterprise search in the life sciences promises to unlock critical clinical and regulatory knowledge. The reality is a high-stakes bottleneck. A typical platform might return hundreds of results for a single pharmacovigilance query, only to bury a critical safety signal on page twelve because it cannot distinguish “cardiac toxicity” (a clinical finding) from “cardiac monitor” (a medical device).
The search technically works. The retrieval is functionally useless.
This isn’t just a failure of relevance ranking; it’s an architectural limitation. Clinical trial protocols, regulatory submissions, and safety filings carry a density of synonyms, abbreviations, and context-dependent terminology that standard keyword searches were never built to interpret. When missing a single document means a delayed IND submission or an unreported adverse event, the gap between “searching” and “finding” transitions from a minor IT nuisance into a severe compliance and operational liability.
Why Do Enterprise Search Tools Fail on Clinical Trial Documents?
The root cause is a fundamental mismatch between how these tools work and how clinical knowledge is structured. Traditional enterprise search platforms rely on keyword matching and Boolean logic. They index words, not meaning. When a researcher queries “treatment-emergent adverse events,” the system matches those exact tokens. It does not understand that “TEAEs,” “treatment-related AEs,” or “drug-induced side effects” refer to the same concept.
Clinical and regulatory documents compound this problem in several ways. First, medical terminology is dense with synonyms, abbreviations, and acronymic variations. A single condition like myocardial infarction might appear as “MI,” “heart attack,” “acute coronary syndrome,” or “STEMI” across different documents in the same repository. According to the National Library of Medicine, the UMLS Metathesaurus alone maps over 4.4 million concept names across more than 200 source vocabularies. No keyword index can account for this breadth of terminology without a contextual layer.
Second, regulatory submissions follow rigid structural conventions (ICH CTD format, eCTD modules) where identical terms carry different meanings depending on the section. “Safety” in Module 2.7 (Clinical Summary) refers to patient-level adverse event data. “Safety” in Module 3.2 (Quality) refers to product stability testing. A keyword search treats both identically.
How Search Tools Miss Context in Regulatory Submissions
Context loss in standard regulatory document search occurs at three distinct levels:
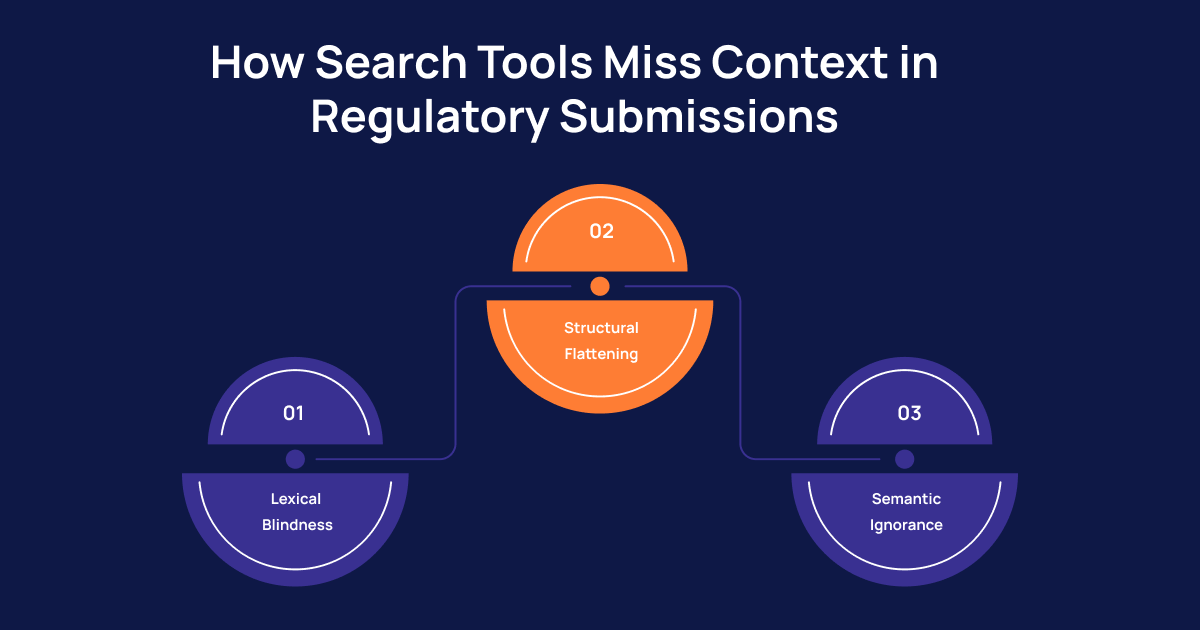
- Lexical Blindness (The Word Level): Keyword engines break compound medical terms into isolated tokens. "Non-small cell lung cancer" becomes four separate words. Consequently, a search may return irrelevant results about "cell culture" or "small molecule" compounds that have nothing to do with oncology.
- Structural Flattening (The Document Level): A 500-page NDA submission has a precise information architecture—clinical study reports nested within safety summaries, cross-referenced to statistical analysis plans. Standard enterprise tools flatten this hierarchy during indexing. When that structure is stripped away, the relationship between a safety finding and its supporting statistical evidence is completely lost.
- Semantic Ignorance (The Meaning Level): Life sciences search requires an understanding of negation ("no evidence of hepatotoxicity" vs. "evidence of hepatotoxicity"), temporal qualifiers ("prior to treatment" vs. "following treatment"), and conditional logic ("if creatinine exceeds 2x ULN, discontinue"). Standard information retrieval systems treat these as equivalent because the core keywords overlap perfectly.
Why Is Metadata Not Enough for Document Retrieval in Regulated Industries?
A common response to search failures is to invest in better metadata tagging. While metadata improves filtering (by document type, study phase, therapeutic area), it cannot solve the core document retrieval problem for two reasons.
First, the volume and velocity of unstructured data in pharma R&D make comprehensive manual tagging impractical. Today, an estimated 80% to 90% of all enterprise data is unstructured. For a mid-size pharma company managing thousands of clinical study reports, investigator brochures, and post-market surveillance filings, maintaining accurate metadata at scale is a resource drain that never reaches completeness.
Second, metadata captures attributes (author, date, document type) but not meaning. A metadata tag can label a document as “Phase III Clinical Study Report.” It cannot tell you whether that report contains a specific subgroup analysis for patients over 65 with renal impairment. The actual intelligence lives in the unstructured narrative, tables, and appendices within the document.
The Shift from Keyword Search to Semantic Search in Healthcare Documents
Semantic search for pharma represents a foundational shift in how clinical document search operates. Instead of matching tokens, semantic engines use vector embeddings to represent the meaning of queries and document passages in a shared mathematical space. A query for “cardiac safety signals in elderly patients” retrieves passages about “cardiovascular adverse events in geriatric populations” because the underlying meaning vectors are proximate, even though no keywords overlap.
This approach directly addresses the synonym, abbreviation, and contextual challenges that break keyword search. When combined with domain-specific training on medical ontologies (MedDRA, SNOMED CT, WHO-ART), semantic retrieval healthcare systems achieve significantly higher precision and recall on clinical corpora than general-purpose search tools.
RAG for life sciences (Retrieval-Augmented Generation) takes this further. A RAG architecture pairs semantic retrieval with a generative model that can synthesize answers grounded in the retrieved source documents. Instead of returning a list of 2,000 links, the system returns a direct answer: “Cardiac toxicity signals were observed in Study XYZ-301 (Module 5.3.5.3), primarily in patients aged 65+ with pre-existing QTc prolongation. See Table 14.3.1 for incidence rates.” The answer includes traceable citations back to the source, which is critical for GxP compliance and audit readiness.
How Intuceo Solves Contextual Search for Clinical and Regulatory Content
Intuceo’s approach to AI search in healthcare is built on a simple reality: generic enterprise search was never designed for the complexity of regulated content. Through two proprietary, modular engines, Intuceo delivers contextual search for regulated content at scale.
Intuceo-Ix™: Neural Search Intelligence (The Discovery Layer)
Intuceo-Ix™ goes beyond keyword matching to provide Neural Semantic Discovery. It understands the true context of clinical papers, regulatory submissions, FDA filings, and patent documents—reducing information retrieval time by 70%.
- Unified Knowledge Layer: Ix indexes and harmonizes data across fragmented silos (SharePoint, LIMS, PLM, clinical trial databases).
- Sub-Second Precision: The InsightExplorer™ interface enables researchers to execute complex, multi-faceted queries across millions of records instantaneously.
- The Business Impact: Knowledge workers who previously spent 90% of their research time on manual information discovery can shift that to 10%, directly accelerating regulatory submission cycle times and freeing capacity for higher-value scientific analysis.
Intuceo-Dx™: Document and Vision Intelligence (The Ingestion Layer)
Intuceo-Dx™ addresses the critical upstream problem: converting complex, unstructured clinical documentation into structured, searchable “Gold Records.”
- Advanced Vision AI: Dx extracts high-fidelity metadata from handwritten clinical notes, lab reports, and legacy regulatory filings that traditional OCR completely misses.
- Traceable RAG Extraction: Its RAG-enabled capability allows teams to query their entire document library as if it were a live expert, ensuring every generated response is perfectly traceable back to its exact source document.
Built for Regulated Environments
Both Ix and Dx are deployable in air-gapped, on-premise, or private cloud environments (IL5/FedRAMP-ready). No proprietary data is used to train public models. This sovereign architecture, combined with compliance alignment for HIPAA, GxP, and 21 CFR Part 11, makes Intuceo’s document intelligence for pharma suitable for the most security-sensitive life sciences organizations.
Conclusion
The gap between what enterprise search tools deliver and what life sciences organizations actually need is not a minor inconvenience. It is a structural problem that affects research velocity, regulatory compliance timelines, and the quality of safety decisions. Keyword matching was built for general corporate content, not for the terminological density, structural complexity, and compliance rigor of clinical trial document retrieval and regulatory document search.
Closing this gap requires a shift to semantic search for life sciences, purpose-built for the domain, deployed in compliant environments, and architected to deliver traceable, contextual answers rather than keyword-matched links. For organizations ready to make that shift, the difference is not incremental. It is the difference between searching for information and actually finding it.
See How Intuceo Transforms Clinical Document Search
Discover how Intuceo-Ix™ and Intuceo-Dx™ reduce information retrieval time by 70% across millions of clinical and regulatory documents, all within HIPAA and GxP-compliant environments.
Frequently Asked Questions
1.What is the difference between keyword search and semantic search in healthcare documents?
Keyword search matches exact terms in a query against indexed tokens in a document. Semantic search for life sciences uses vector embeddings to match the meaning of a query to the meaning of document passages, enabling accurate retrieval even when the exact words differ. This is critical for medical terminology search, where synonyms, abbreviations, and acronyms are pervasive.
2.How can AI search understand medical terminology and synonyms?
AI-powered semantic retrieval healthcare systems are trained on domain-specific ontologies such as MedDRA, SNOMED CT, and UMLS. This training allows the system to recognize that “MI,” “myocardial infarction,” and “heart attack” refer to the same clinical concept, enabling synonym matching in medical documents that keyword engines cannot achieve.
3.How do enterprise search systems handle abbreviations in life sciences?
Most conventional systems do not handle them well. Abbreviations like “AE” (adverse event), “SAE” (serious adverse event), and “TEAE” (treatment-emergent adverse event) are either missed or conflated with unrelated acronyms. Neural search systems trained on life sciences corpora resolve these abbreviations contextually, based on the surrounding text and document type.
4.How do you improve semantic search for clinical knowledge bases?
Three elements drive improvement: domain-specific model fine-tuning on clinical and regulatory corpora, integration with established medical ontologies for entity resolution, and a RAG for life sciences architecture that grounds every retrieved result in verifiable source documents. This combination ensures both precision and auditability.
5.What causes irrelevant results in pharma document search?
Irrelevant results stem from three gaps: lexical ambiguity (the same word meaning different things in different contexts), structural flattening (loss of document hierarchy during indexing), and semantic blindness (inability to interpret negation, temporal qualifiers, and conditional statements). Addressing all three requires moving from token-based to meaning-based information retrieval.