Predictive and explainable models stop at the score. The capability that changes outcomes is prescriptive: knowing which factors a team can act on, and the shortest path from a bad outcome to a better one.
Health systems can now flag, with reasonable accuracy, which patients are likely to return within 30 days of discharge. The models work. The readmission rate has not moved with them. The 30-day all-cause readmission rate held at about 13.9 per 100 index admissions between 2016 and 2020, reaching 17.0 per 100 for Medicare patients.1 A prediction arrived. The outcome stayed the same.
The reason is rarely the model. It is the gap between knowing what will happen and knowing what to change.
Prediction stalls at the score
Most machine learning systems are built to answer one question. What will happen? This customer will churn. This loan will default. This patient will be readmitted. That answer is useful, and it is also where most systems stop.
Decision-makers cannot act on a probability. A clinical director looking at a readmission score still needs several things that the score does not provide. Why is this patient at risk? Which of the contributing factors can the care team actually influence? What is the smallest change that would lower the risk? And of all the available options, which is the shortest, most feasible route to a better outcome?
A risk score answers none of these. It ranks cases. It does not specify what action needs to be taken. The result is a model that earns its place in a report and never reaches the call list, the discharge plan, or the workflow where the decision gets made.
Explanation is not the same as action
Explainable AI was supposed to close this gap. It helps, but it does not finish the job. Feature attribution tells a team which variables are associated with an outcome. It says that low engagement and unresolved complaints correlate with churn, or that prior admissions, medication complexity, and social factors correlate with readmission.
Knowing what is associated with an outcome is not the same as knowing what to do about it. A real decision system has to separate several different kinds of attributes:
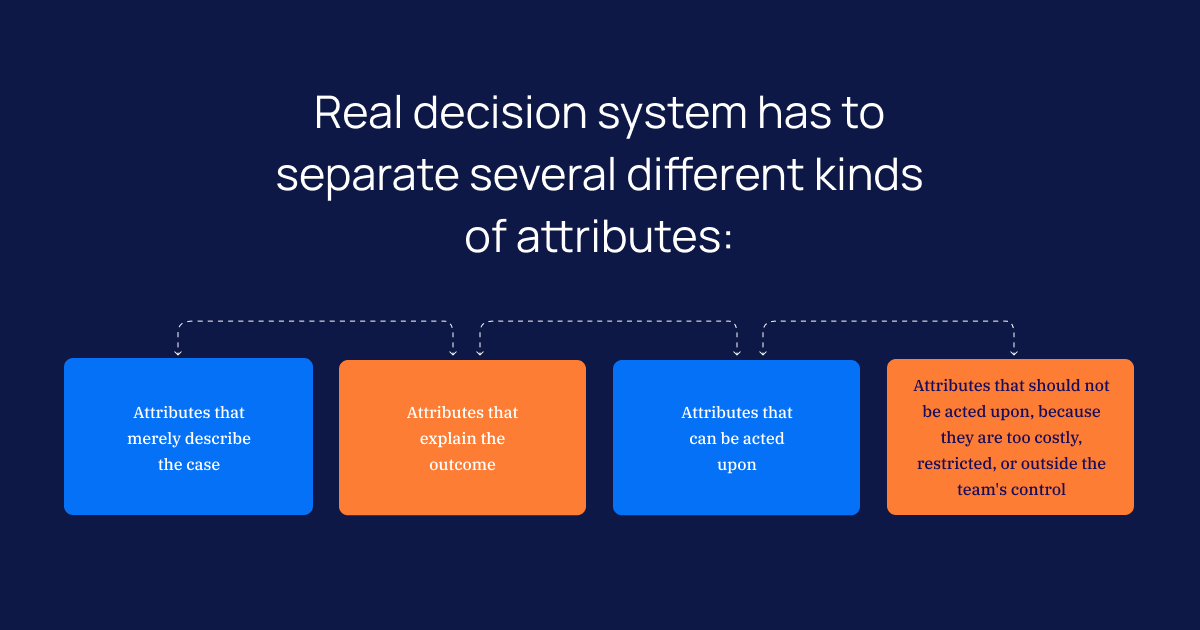
- Attributes that merely describe the case
- Attributes that can be acted upon
- Attributes that should not be acted upon, because they are too costly, restricted, or outside the team's control
A patient’s age explains readmission risk, and it cannot be changed. A medication reconciliation step at discharge also influences risk, and it can be changed this afternoon. An explanation that treats both as equally important sends the team nowhere. The intelligence is in the distinction.
What prescriptive intelligence actually requires
The capability that closes the gap is prescriptive. It does more than score and explain. It identifies the specific, feasible changes that move a case from an undesired state to a desired one, and it ranks those changes by impact, effort, and constraints.
Three things have to work together for that to happen. Rule extraction pulls the decision logic out of high-dimensional data instead of leaving it locked inside a black box. Actionable attribute selection separates the factors a team can change from the ones it cannot. Shortest-path reasoning finds the minimal set of changes that produces the result, rather than handing over a list of fifty possible interventions.
That last point carries more weight than it first appears. Decision-makers do not want a hundred recommendations. They want the smallest change that moves the needle: the one process fix that prevents a delay, the single follow-up that keeps a patient out of the hospital, the behavioral shift that moves a case into a safer class. Listing every possible intervention is easy. Ranking the feasible ones by what they cost and what they return is the hard part, and it is where the value sits.
A worked example: the high-risk patient
Illustrative scenario
A discharge planner looks at a patient the model has flagged as high-risk for readmission. An explanation layer lists the drivers: multiple chronic conditions, a complex medication regimen, a missed prior follow-up, and limited transport to appointments.
The planner still has to decide what to do before the patient leaves. Several of those drivers are fixed. The chronic conditions are not changing this week. But the medication regimen can be reconciled and simplified now. A follow-up can be scheduled and confirmed. A transport barrier can be answered with a referral.
A prescriptive system does not stop at the four drivers. It identifies which are modifiable, which are feasible given the team’s resources, and which combination forms the shortest path to a lower risk. That is the difference between a model that produces a number and a system that produces a decision.
Why prescriptive paths are also a governance asset
In regulated industries, a recommendation is only useful if it can be defended. A clinical or compliance reviewer has to ask whether a recommendation is justified, whether it can be audited, whether a domain expert would validate it, and whether it is fair and operationally feasible.
Black-box predictions struggle with every one of those questions. A transformation path does not. Because it is built from extracted rules and a stated sequence of changes, it can be inspected, challenged, and approved before anyone acts on it. The same structure that makes a recommendation useful to a care team is what makes it defensible to a regulator. In healthcare, life sciences, and other high-stakes settings, that is not a feature. It is a requirement.
From prediction to prescription
The lesson holds across every model an enterprise runs. A predictive model says something is likely to happen. An explanatory model says which factors are associated with it. Neither tells the organization what to change, in what order, with the least effort, to improve the outcome. That last step is where measurable value lives.
This is the principle behind Intuceo’s approach to decision intelligence. The Intuceo-Ax engine pairs prediction with a Rationalization Layer that surfaces the statistical evidence and logic behind a recommendation, instead of a yes or no answer. In adverse event reporting and risk stratification, that means a model does not just predict, it justifies, which is what regulatory frameworks like GxP and HIPAA demand. The work is delivered as explainable, governed systems, built and validated through the iPDLC development framework, rather than a black box dropped into a workflow.
Prediction was never the finish line. The organizations that see returns from AI are the ones that treat the score as the start of a decision, not the end of one.
There is a harder question waiting in the GenAI era. If models like GPT and Claude can reason and explain so fluently, why can’t they deliver this structured, auditable path on their own? That is the subject of the next post.
Turn predictive models into decisions your teams can act on.
Intuceo builds explainable, governed decision intelligence for healthcare, life sciences, and other regulated industries.
Frequently Asked Questions
1.What is the difference between predictive and prescriptive analytics?
Predictive analytics estimates what is likely to happen, such as which patients may be readmitted or which loans may default. Prescriptive analytics goes further. It identifies the specific, feasible changes that move a case toward a better outcome, then ranks them by impact, effort, and constraints, so teams know what to do, not just what to expect.
2.Why isn't explainable AI enough to act on a prediction?
Explainable AI shows which factors are associated with an outcome, but association is not action. A useful system also has to separate the factors a team can change from those it cannot, such as a patient’s age versus a discharge medication review. Prescriptive intelligence adds that distinction and finds the shortest path to a better result.
3.Can prescriptive AI recommendations meet regulatory requirements like HIPAA or GxP?
Yes, when the recommendation is built from extracted rules and a stated sequence of changes rather than a black-box score. That structure can be inspected, challenged, and validated by a domain expert before anyone acts, which is what frameworks such as HIPAA and GxP require. A transparent rationalization layer makes the recommendation defensible, not just accurate.